Oral Habits and Teeth Alignment: A Parent’s Guide
May 22, 2026
Oral Habits and Teeth Alignment: A Parent’s Guide
TL;DR:
- Childhood oral habits like thumb sucking and mouth breathing can cause significant jaw and teeth misalignment if left unchecked during critical development years. Early identification and professional intervention are essential to prevent complex treatments later, as these habits directly influence craniofacial growth and function. Addressing these behaviors through behavioral, environmental, and orthodontic strategies improves long-term oral health and facial development.
Most parents assume that childhood habits like thumb sucking or mouth breathing are phases kids simply grow out of. The reality is more complicated. The connection between oral habits and teeth alignment is well-documented, and the window during which habits cause the most damage often overlaps exactly with the ages when permanent teeth are erupting. If your child is between 7 and 12, this is the period that matters most. Understanding how everyday habits silently reshape developing jaws and teeth gives you the chance to act before correction becomes significantly harder.
Table of Contents
- Key Takeaways
- Common oral habits that affect teeth alignment
- How oral habits lead to teeth alignment issues
- Identifying harmful habits early and when to get help
- Strategies to manage and correct detrimental habits
- Orthodontic treatment options for habit-related misalignment
- My honest take on the “they’ll grow out of it” myth
- How Gloworthodontics can help your child’s smile
- FAQ
Key Takeaways
| Point | Details |
|---|---|
| Habits cause real structural change | Oral habits like thumb sucking and tongue thrusting directly alter jaw shape and tooth position during development. |
| 100% malocclusion link confirmed | Children with oral habits universally show malocclusion, with dramatically higher orthodontic treatment needs. |
| Early identification is the leverage point | Recognizing habits before age 7 to 8 gives orthodontists and parents time to redirect development without complex treatment. |
| Behavioral and professional tools both matter | Combining positive reinforcement at home with professional myofunctional therapy or early appliances produces better outcomes. |
| Treatment choice depends on habit severity | Severe malocclusion caused by prolonged habits often requires braces over clear aligners for precise correction. |
Common oral habits that affect teeth alignment
Children develop oral habits for many reasons: soothing anxiety, boredom, or simple repetition. The habits that draw the most attention from orthodontists include thumb sucking, pacifier use, mouth breathing, tongue thrusting, nail biting, lip chewing, and bruxism (grinding teeth during sleep). Each one exerts a different type of force on teeth, jaw bones, and the surrounding muscle tissue.
What determines how much damage occurs is not just the habit itself, but three factors: frequency, duration, and intensity. A child who sucks their thumb occasionally while falling asleep is very different from one who maintains suction for hours throughout the day. The more sustained the pressure, the greater the effect on bone and tooth positioning.
Here is what each major habit tends to produce:
- Thumb sucking and pacifier use: Forward pressure on upper front teeth and inward pressure on lower teeth, leading to an anterior open bite or posterior crossbite
- Mouth breathing: Altered tongue posture forces the tongue down and forward, disrupting normal palatal development and leading to a narrow upper arch
- Tongue thrusting: Constant forward tongue pressure against teeth during swallowing, contributing to open bite and speech development issues
- Nail biting: Creates micro-fractures in enamel over time and places asymmetric forces on specific teeth, generating TMJ stress
- Lip chewing and sucking: Pulls lower front teeth inward and pushes upper teeth outward, worsening overjet
- Bruxism: Wears enamel flat and creates bite imbalances that shift teeth out of position gradually
Pro Tip: Watch your child during screen time and sleep. These are the periods when unconscious habits are most active. A quick five-minute check while they are watching TV or relaxing can reveal habits they are not even aware of themselves.
How oral habits lead to teeth alignment issues
Understanding why these habits cause problems requires a brief look at how developing jaws work. During childhood, the bones of the face and jaw are still soft and responsive to pressure. Sustained muscle forces, even gentle ones applied repeatedly, reshape bone over time. This is actually the same principle that makes orthodontic treatment work. The difference is that habit-driven forces are uncontrolled and often asymmetric.
The three most common malocclusion types linked to oral habits are anterior open bite, posterior crossbite, and increased overjet. An anterior open bite occurs when upper and lower front teeth cannot meet, leaving a visible gap. A posterior crossbite means upper back teeth sit inside the lower teeth rather than outside. Increased overjet refers to upper front teeth that jut too far forward.
Mouth breathing specifically causes maxillary constriction, increased facial height, and altered occlusal development by changing the resting position of the tongue and disrupting the normal balance of muscle forces around the upper arch.
| Habit | Primary malocclusion risk | Supporting evidence |
|---|---|---|
| Thumb sucking | Anterior open bite, increased overjet | High correlation with prolonged use beyond age 4 |
| Pacifier use | Posterior crossbite | OR 2.66 for crossbite in pacifier users |
| Mouth breathing | Narrow upper arch, long face pattern | Linked to maxillary constriction |
| Tongue thrusting | Anterior open bite, spacing | Associated with open bite and speech issues |
| Nail biting | TMJ stress, enamel wear | Asymmetric bite forces on specific teeth |
Children with deleterious oral habits universally exhibit malocclusion, and 31.6% require high-level orthodontic intervention compared to just 2.4% of children without habits.
The data makes clear that these are not cosmetic concerns. The impact of oral habits on craniofacial structure extends to breathing function, speech, and long-term jaw health.
Identifying harmful habits early and when to get help
The earlier you catch a habit, the less structural correction is needed later. Most orthodontists use age 5 to 6 as the threshold where habits shift from “watch and wait” to “take action.” By the time a child is 7 or 8 and permanent teeth are coming in, a habit that persists is actively competing with normal development.
Here are the signs that a habit is affecting your child’s teeth alignment:
- Visible gaps between front teeth when the mouth is closed at rest
- Upper teeth that flare forward noticeably beyond the lower lip
- A narrow or high-arched palate, which you can observe by asking your child to open wide
- Open mouth posture at rest, particularly during sleep or concentration
- Snoring, restless sleep, or daytime fatigue, which may indicate sleep-disordered breathing. 10 to 15% of children are affected by sleep-disordered breathing, and mouth breathing is a primary driver
- Speech difficulties such as a lisp, which can signal tongue thrusting patterns
If you observe any of these signs consistently, schedule a dental or orthodontic evaluation. The Pediatric Sleep Questionnaire is one clinical screening tool that dentists use to flag breathing-related habits, but any qualified orthodontist can assess your child’s occlusion and identify habit-related changes during a routine exam. Early screening within an orthodontic assessment enables timely referrals and prevents worsening alignment.
Pro Tip: Keep a simple habit log for two weeks before your child’s dental appointment. Note when you observe the habit, how long it lasts, and what your child is doing at the time. This information helps a clinician distinguish between an occasional soothing behavior and a structural risk.
Strategies to manage and correct detrimental habits
Stopping a habit cold is rarely the right approach, especially with younger children. The most effective strategies combine behavioral support, environmental changes, and professional guidance.
Behavioral strategies work best when they replace the habit with something else rather than simply punishing it:
- Use positive reinforcement charts where your child earns a reward for habit-free days
- Remind without shaming. A gentle physical cue, like placing your hand briefly on theirs, can redirect thumb sucking without creating anxiety around it
- Discuss the habit openly with your child. Children aged 7 and older often respond well when they understand the effect on their teeth
- Identify triggers. If the habit spikes during homework or screen time, introducing a fidget tool or a different activity during those periods can reduce frequency
Environmental modifications address the physical dimension:
- Keep fingernails short and clean, which reduces the sensory satisfaction of nail biting
- Use a bitter-tasting nail polish designed to discourage biting in children
- Address sources of stress or anxiety at school or home, since many habits intensify with emotional tension
Professional treatments become necessary when behavioral approaches are not enough:
- Myofunctional therapy trains the tongue, lips, and facial muscles to rest and function in positions that support normal alignment
- Habit-breaking orthodontic appliances, such as a tongue crib or palatal arch, create a physical barrier that interrupts the habit
- Early orthodontic consultation opens the door to interceptive treatment, which can guide jaw development before permanent teeth are fully in place
The benefits of addressing crooked teeth causes early extend beyond appearance. Oral habits affecting smile development and speech are easier to correct when the jaw is still growing and responsive.
Orthodontic treatment options for habit-related misalignment
Once a habit has already caused teeth alignment issues, treatment planning depends on the severity of the malocclusion, the age of the child, and whether the habit has been resolved.
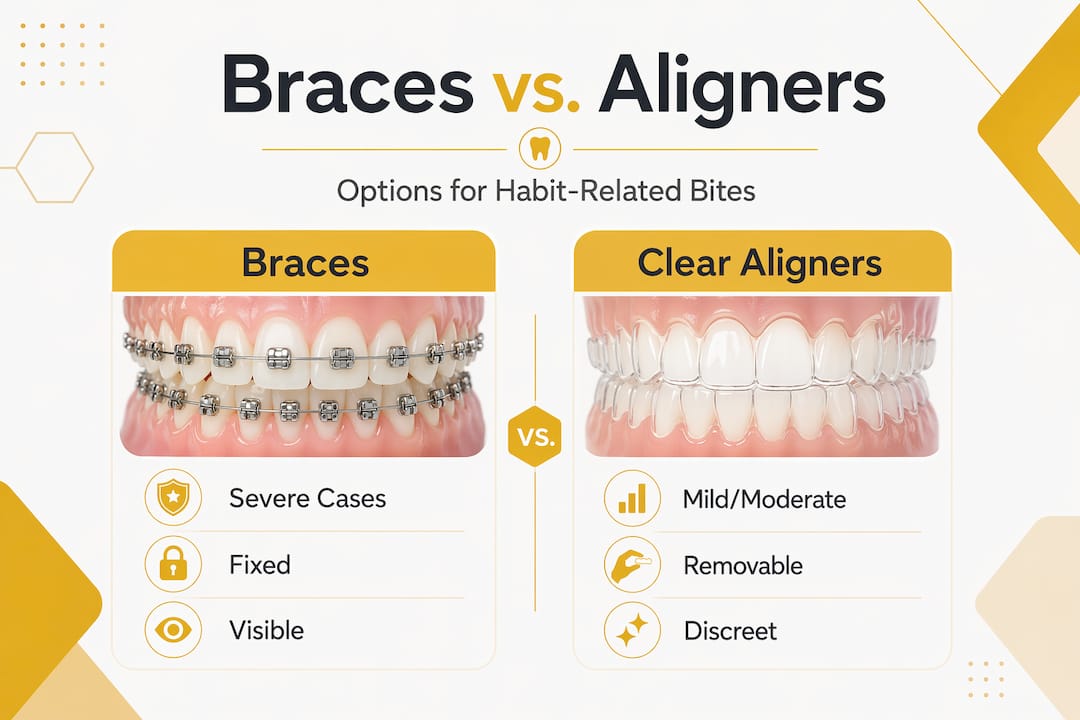
Braces vs. clear aligners
Braces are more effective for severe malocclusions, particularly those involving significant bone changes from prolonged habits. They provide continuous, precise force and do not rely on patient compliance for wear time, which matters with younger children. Clear aligners work well for mild to moderate problems and are a realistic option once the habit is fully stopped and most permanent teeth have erupted.
| Factor | Braces | Clear aligners |
|---|---|---|
| Severity of malocclusion | Severe and complex cases | Mild to moderate cases |
| Patient compliance needed | Lower (fixed in place) | High (worn 20 to 22 hours daily) |
| Habit interference | Unaffected by ongoing habits | Can be disrupted if habit persists |
| Best age for children | From ages 7 to 8 onward | Typically 11 and older |
| Complex bite correction | Strong capability | Limited in severe bite cases |
One factor parents often overlook is gum and tissue health. Periodontal stability is a prerequisite for safe orthodontic tooth movement. Children who have been mouth breathing for years may have gum inflammation that needs addressing before treatment begins. An orthodontist may refer you to a periodontist before starting active treatment if tissue health is a concern.
Pro Tip: Ask your orthodontist specifically about the differences between braces and Invisalign before committing to a treatment plan. The right choice depends heavily on what habits your child had, how long they persisted, and what the current state of their bite is.
My honest take on the “they’ll grow out of it” myth
I have seen it happen more times than I can count. A parent brings in a ten-year-old with a significant open bite, and when asked about thumb sucking or mouth breathing, the response is almost always the same: “We thought they’d stop on their own.”
The belief that children naturally outgrow oral habits is not wrong in every case. Many do stop. The problem is that parents and even some general dentists tend to apply this “wait and see” approach well past the point where it is safe to wait. By age 7 or 8, permanent teeth are arriving and the jaw is actively laying down bone structure. Every month a habit continues past that point is a month of unchecked force shaping a developing skull in the wrong direction.
What I find even more overlooked is the connection between sleep-disordered breathing and behavioral issues, including attention difficulties. Children who mouth breathe at night are frequently poor sleepers, and poor sleep mimics or worsens ADHD-type behaviors. Orthodontists, pediatricians, and parents rarely connect these dots early enough. Addressing the breathing habit through orthodontic or myofunctional intervention can have effects that go far beyond teeth alignment.
The cases I have seen with the best outcomes share one thing in common. Someone noticed the habit early, took it seriously, and got a professional involved before the window closed. That is not fearmongering. That is just how child development works.
— Juiced
How Gloworthodontics can help your child’s smile
If you have been reading through this article and recognizing your child in the descriptions, the next step is a professional evaluation, not more waiting.
At Gloworthodontics, families in the Langley, BC area receive thorough orthodontic assessments that include habit screening and personalized treatment planning for children at every stage of dental development. Whether your child needs early interceptive treatment, myofunctional guidance, or is ready for full orthodontic care, the team at Gloworthodontics works with you and your child to find the right fit. Explore your options with the orthodontic care family guide or compare Invisalign vs. braces to understand what treatment might look like. Book a consultation at gloworthodontics.ca and start the conversation today.
FAQ
Can oral habits actually change a child’s jaw shape?
Yes. Sustained pressure from habits like thumb sucking and mouth breathing reshapes developing bone over time. The jaw is most responsive during the ages of 6 to 12, making this the period of greatest risk.
At what age should a parent seek help for an oral habit?
Most orthodontists recommend evaluation by age 7. Habits that persist beyond age 5 to 6 carry a measurable risk of causing teeth alignment issues, particularly as permanent teeth begin to erupt.
Do all children with oral habits need orthodontic treatment?
Research shows that children with oral habits universally develop some form of malocclusion, but treatment intensity varies. Catching habits early and stopping them reduces the severity of correction needed.
Is mouth breathing really a dental problem or just a breathing one?
It is both. Chronic mouth breathing alters tongue posture, narrows the upper arch, and disrupts normal dental occlusion. It also affects sleep quality and can contribute to behavioral and learning difficulties in children.
Are clear aligners a good option for children with habit-related bite problems?
Clear aligners work well for mild to moderate cases, but severe misalignment caused by prolonged habits typically requires braces for precise correction. An orthodontic evaluation will determine which approach suits your child’s specific situation.